Draft Rev 1
In my recent round of meeting San Francisco's Healthcare and Biotech Venture Capitalists, a comment made by one particular investor stuck with me:
"Behavior change is the hardest part about health." -[redacted]
In the context of our conversation this meant:
A core measure of an intervention's success is whether patients follow through with treatment
A general method for influencing behavior is highly valuable (especially to payors)
While there is nothing novel here, I think his remark helps us refocus on the fundamentals. It is easy to get excited about a new miracle drug or sophisticated diagnostics tools, but the fundamental problem in healthcare is changing and sustaining new habits.
Two fields have focused intently on behavior change, Consumer Goods and Education.
Consumer:
There are some spiritual traditions in which your Guru passes down a mantra. The mantra is a powerful phrase to be repeated and kept secret.
At risk of it losing its power and disgracing my Guru, I'll divulge the mantra I have internalized this past year. "LTV to CAC"
I spent the last year researching and starting a consumer company. At first spinning up SomaticDesign.us and then working at Base Power to see what ops at scale look like.
Many sleepless nights were spent anxiously thinking about Brand Positioning and testing in public to validate.
To be contd. explanation of how a consumer approach is crucial to creating the best healthcare experience.
Education
What can The Alexander Technique and an understanding of inhibition teach us about actual methods for behavior change?
To be contd.
Draft Rev 2
"I have back pain" is a common phrase. Most people who say this have low back pain, but a number of people also refer to their upper back, perhaps that area between their spine and shoulder blades.
Why do people have back pain? Maybe an acute injury - auto accident/sports. Or perhaps misuse of their body over time - posture, poor movement habits. The body is adaptable, and most things go away with some rest and regular movement. But the pain that doesn't go away can for some turn chronic, and become quite inhibiting in their life.
The usual course of action is to go to your PCP, who might refer you to an ortho for some imaging - xray + mri to see if something is obviously mechanically off. And then you might go to a PT, who will usually do an evaluation and prescribe exercises.
In my case, and in many other cases, this path doesn't work. Imaging doesn't pick up on anything abnormal, but pain persists. PT prescribes exercises, but you don't fully understand why and they don't seem to be targeting the root cause.
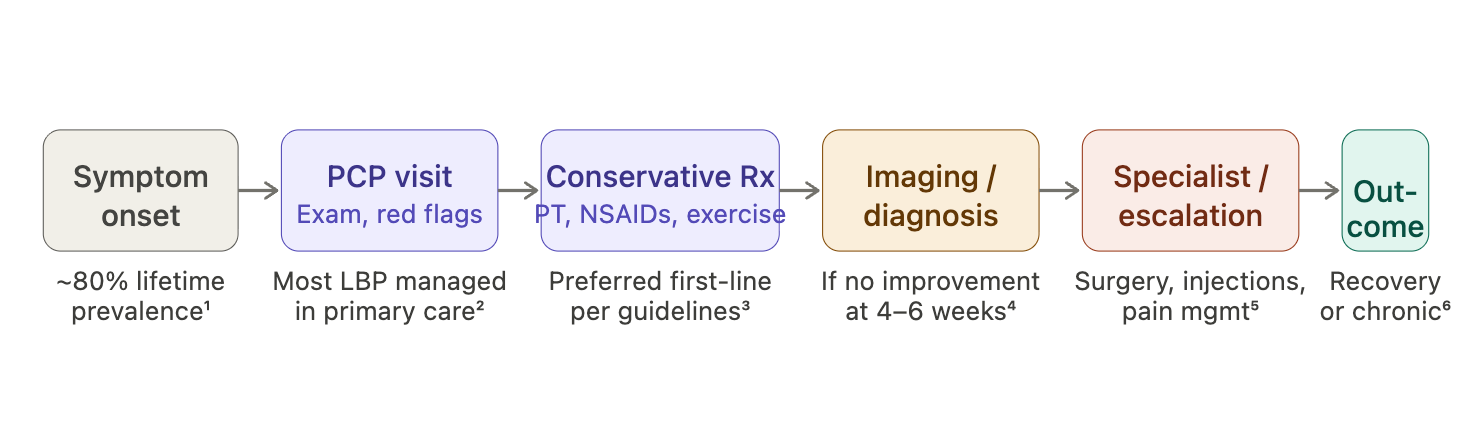
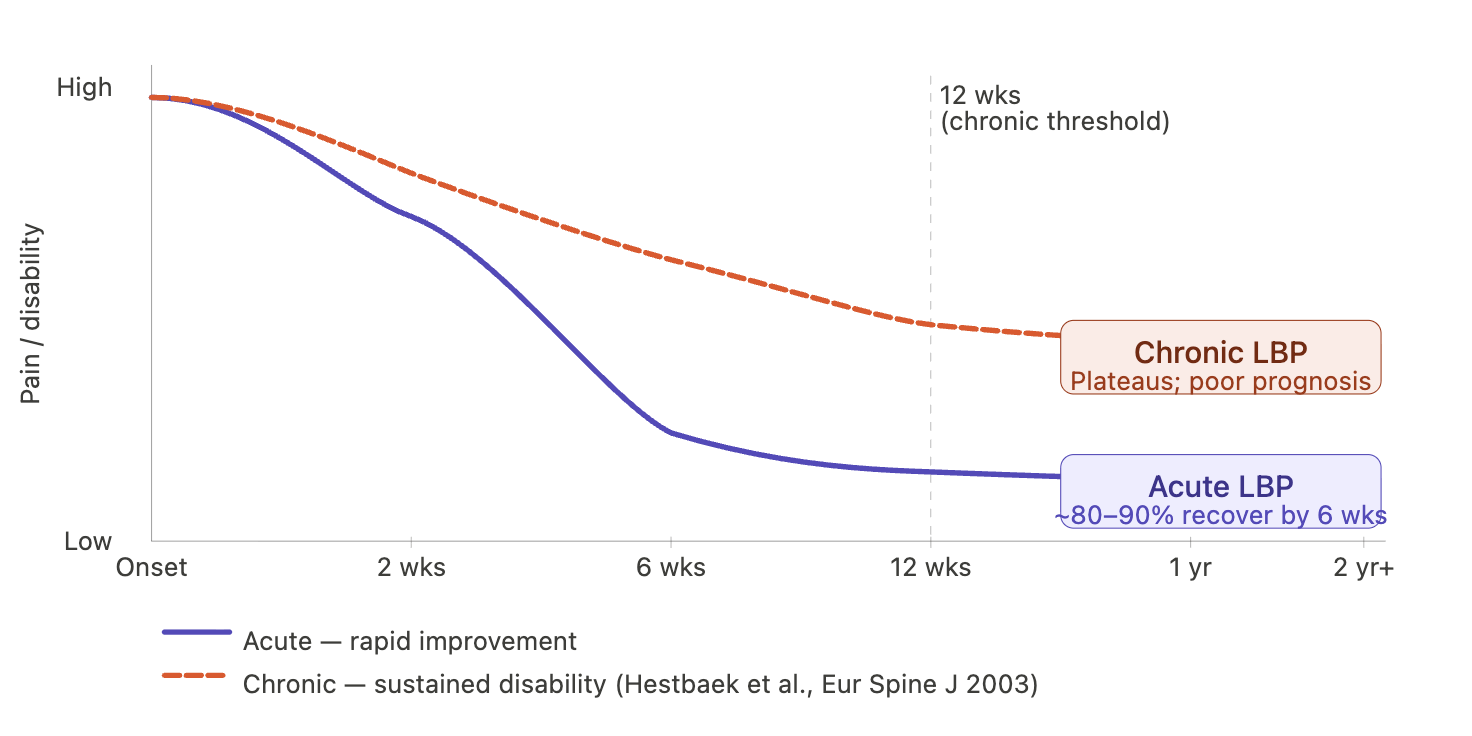
The standard clinical flow for an individual experiencing "low back pain" is diagrammed below. It is usually after seeing a physical therapist and one specialist (~12 weeks) that the population drops off into a chronic pain category.
First it is important to define clbp. The "low back" is quite a vague region. In the area are the SI joints, lumbar vertebrae, and a little further out - the hip joints. Realizing that there is a front to the low back, we encounter our lower intestines, and key muscles like the psoas. So when someone reports low back pain, how exactly can we specify the site of pain and its cause?
The nervous system is deeply entangled in pain, and as of late has received more attention in pain science. So perhaps we can start there. The lower back is where key nerves leave the spinal column, impingement could be a cause of pain. Vertebrae and joints themselves are innervated, as are local muscles like the glutes or erector spinae, perhaps irritation at or around those areas can be the cause of pain. This is all useful and interesting, but what we are missing is the idea that pain isn't just a clear mechanistic output of injury, our own attention and beliefs can contribute to increased sensitization, poor patterns of movement, and sustenance of pain.

Dysfunction (==clbp==) is a state marked by an experience of pain (==self report==)[^2], and inhibited movement[^3]. If we consider a certain range of motion and type of movement in joints and the body collectively to be the norm, then a deviation is considered dysfunctional. Causes are psychological[^5] and physiological ([[bigos1991.pdf]], [[Biomechanical and Psychosocial Risk Factors for Low Back Pain at Work.pdf]], [[dianostic + classification.pdf]])
Biomechanical Models: https://www.sciencedirect.com/science/article/abs/pii/S136085921600005X
Lets go back to "Why do people have back pain?" Sure there is acute injury or postural issues, but there are also psycho social factors. Many people with chronic pain experience anxiety, some argue that pain is a psychological construct. [[Stanley Bigos]] [[Robert Norman]]
Frankly, all of these models of injury cause can be right, so it is tricky to settle on one exact causal model: social isolation --> poor posture and lack of movement --> improper skeletal load distribution --> low back pain. This is one feasible explanation, but what we really need to remember is that individuals are unique and the causes of their pain can't be generalized.
Stu McGill says something along the lines of "There is no nonspecific back pain"[^4]. Stu himself had a broken pelvis and a limp for much of his life, with a hip replacement at 59. A strong proponent of root causing biomechanical causes of pain, but also admits that there is something magic about bodywork as those practices helped defer his own surgery. The biomechanics legend himself crediting bodywork is reason enough to explore a potential combined approach to MSK treatment.
So what do you do if you are an individual struggling with back pain, or you are a practicioner treating it? The best thing to do is be specific. Understand yourself (or your patient) in depth. Hear their background and story, then physically assess their body. The absurd thing is that most PTs won't even put their hands on their patients to feel what is wrong. Relying on tests and scans can get you so far, but feeling someone's skin and muscle can get you a lot closer to finding out the issue + discovering new ones (patients will speak up about long forgotten injuries on pains when you actually touch them).
So as we've said here, step one is a thorough assessment. A practicioner or individual has both external and internal tools at hand. External tools might be imaging devices, internal is the actual sensation of the body. Then comes the intervention, which should be obvious based on the assessment.
Assessment. Intervention. ==why isn't there more movement analysis in treating pain?==
Current modes of assessment are self reporting (patient history + narrative), imaging (x-ray, MRI), Muscle testing (weakness in certain movements). Less common but very exciting - hands on palpation and bodywork, biomechanical modeling + gait analysis.
Interventions - exercise protocol, e-stim. Less common but very exciting - Alexander technique (body awareness + attention training), bodywork (rolfing - hands on massage), dry needling (targeting innervated tissue to intervene in nervous system), postural education.
This should ideally be a pretty tight feedback loop of experiments. Very experienced practicioners are open minded, use the tools they have for a whole assessment of the individual, and then humbly try different interventions.
[^2]: [[berliner study.pdf]]
[^3]: [[fear avoidance lbp.pdf]]
[^4]: [[The Thinking Practicioner]]
[^5]: [[sarno study.pdf]]
Outstanding questions: What is low back pain? - Amy Bauman What are methods of assessing low back pain? What are clear interventions for low back pain? What does the gold standard of treatment look like for low back pain? What is the healthcare system? What fundamental assumptions or beliefs does our healthcare system build off of?
One of the fundamental questions is how do we understand and treat actual mechanical dysfunction along with the mind induced chronic pain someone might be having?
*Outline*
-entities
-relationships
-incentives
-north stars
Mapping modalities (fundamental philosophies, services offered) and approaches to providing improved access to MSK-health supply.
Beginning with practicioner types and modality overview, ending with business implementation exploration - healthcare models, practicioner matching, supply demand analysis and operations design (platform mechanics).

"Don't even get me started on Value based MSK care, it doesn't work" (Akash, [[2-24-2026.txt]])
Value based care models vs regular insurance schemes for treating patients. In Akash's experience, clinics were optimizing for max number of visits per client and are also incentivized by max return per code charged to insurance.
Kyle is seeing an upwards trend in white collar professionals with low back pain ([[2-22-2026.txt]])
Neil and his experiences with mixed incentives and clinic rollups worsening care.
"Telehealth consolidation represented 22% of 2025's M&A activity, reflecting the shift from general telemedicine toward condition-specific virtual care models 6" (cbinsights).
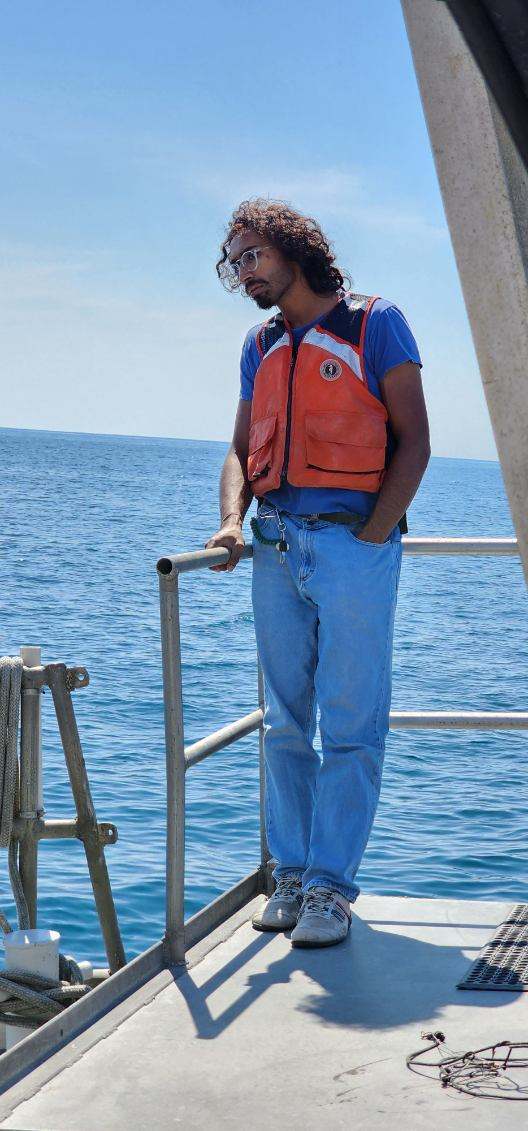
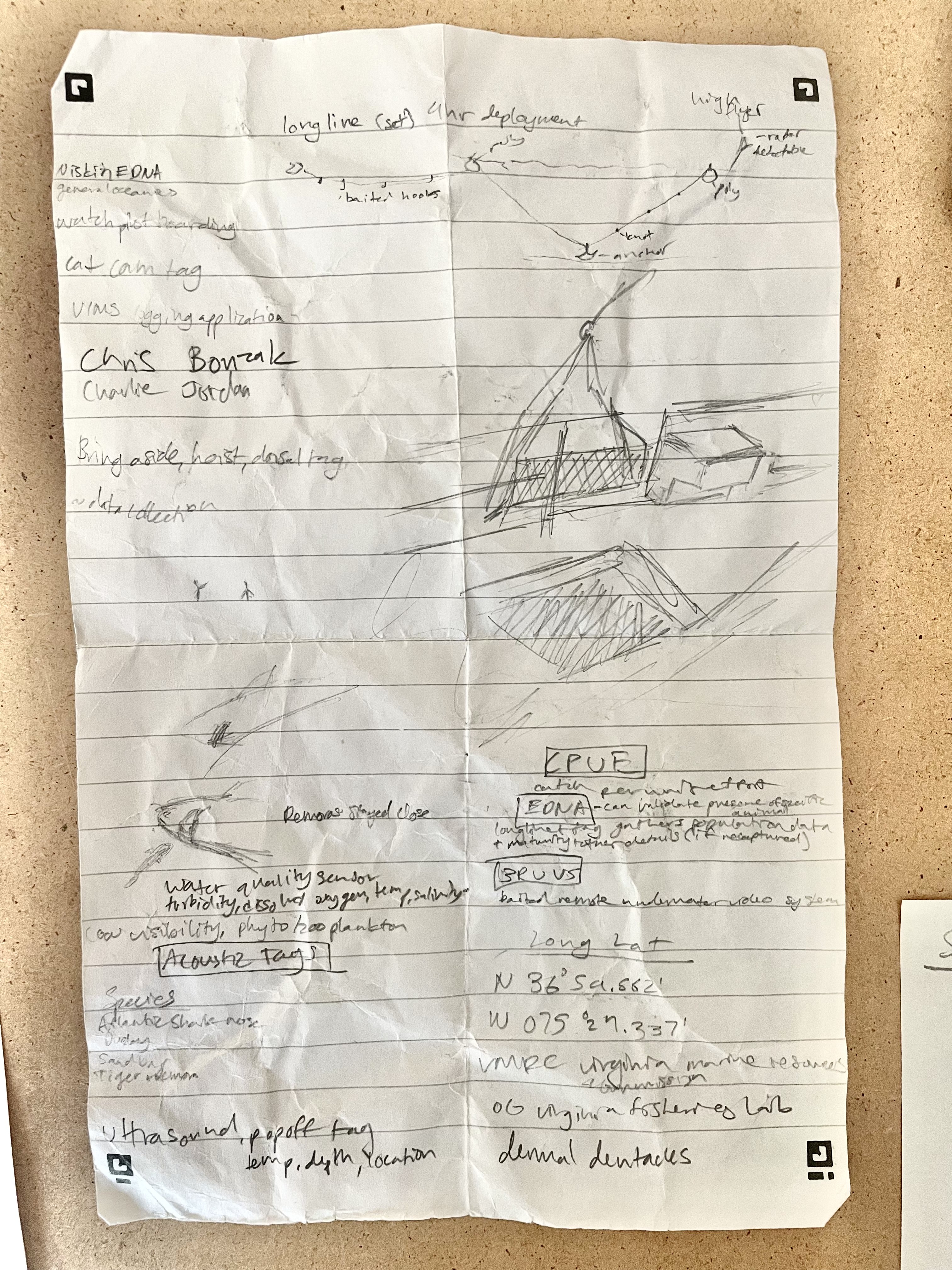
N 36 degrees 59.562 W 075 degrees 24.337 roughly 30 miles off the coast of the Virginia-Carolina border aboard the Virginia Institute of Marine Science Research Vessel:
I peered over the edge of the railing at a several hundred pound Tiger shark we'd hooked. I'd expected to feel excitement, fear paired with adrenaline, but instead I just felt sad. The Tiger was almost catatonic. It floated on its back as the two Remoras it traveled with swam in circles nearby. It hadn't been a fair fight. In fact we'd totally missed the fight. The shark was caught on one of a hundred hooks we'd set out 4 hours prior-we were just now circling back.
One year prior, Paul Clerkin and Miguel Montalvo walked into the Robotics club at William and Mary. I ran the club, and they explained that they wanted something that would streamline the process of tracking marine animals. The current practice of hooking the beast, pulling it on board and then piercing its dorsal fin to tie a tag through was barbaric and outdated. Solution? A non-invasive clip-on shark tag. I was excited, and I got to work. In fact the first time I dropped out of college I was heads down building this tag. But now, on the boat, seeing the process I was getting involved with, I didn't find myself so motivated. This was the beginning of the end of my Marine robotics arc.
I went back to Williamsburg and I wanted to give it another shot. I had built up experience and connections for a potential career as a marine robotics guy. I wanted to know if I could be involved with marine science out of my own love for it. So I rode Ginger's bicycle down to lake Matoaka. I found a secluded spot off the trail and took off most of my clothes. I slowly stepped into the frigid water and tip toed forwards until I was submerged. My feet sunk into the mass of leaves that had settled and begun to decompose on the lake floor. Now with my head submerged I tried to find some personal connection to the lake. Any semblence of love or emotion that could justify my working towards marine robotics. I got out of the water and put my clothes back on. The water was freezing. A week later I spoke with a faculty member who headed research on water quality and the Lake. He told me there were massive alligator Gar in the lake. I didn't care about the lake anymore. It was over, I'd have to find something new.


As a student and as an engineer, I've often been told to forgo the white rabbit in favor of being practical. Its true-it is a tricky dance to entertain your curiosity. The answers you hope for rarely come. Rather, the questions keep evolving. But when you finally sit with your work and reflect, it becomes obvious that the winding path was the straightest possible one.
In my Religious Studies classes I explored Consciousness through multiple philosophical frameworks. In my Computer Science classes I delved into the algorithms foundational to neural networks. At some point early last year, there was much talk of AGI becoming "Conscious". These conversations even made it to the dinner table at Thanksgiving. Suddenly, my seemingly isolated coursework had a clear overlap. I was gripped by this intersection. Could AI become "Conscious"?
In Computer Science, a crucial concept is Abstraction. Tidy up the details of implementation and expose only a stable interface. This is necessary for building adaptable and complex systems. But to answer the question: could AI be conscious required diving deep.
I started by learning C and studying RISC architecture. I read datasheets and wrote firmware for ARM processors so I could directly interface with memory and create a Perceptron. Still, I didn't find any answers about how AI could become "Conscious". So I went deeper. I bought physics textbooks and snuck into Physics classes. I studied Maxwell's equations, Feynman's lectures and Einstein's Relativity. I could calculate field strength at a point, appreciate the elegance of the equations and make use of the water analogy but I still lacked a felt understanding. If electrical signals could somehow make AI "Conscious", I knew I had to build an intuition. So I designed an instrument. I wanted to hear, feel and see electricity.
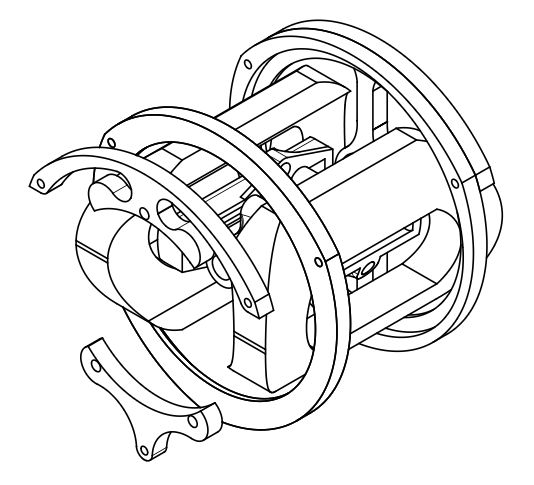
Below is that instrument and a snippet of sound I just recorded. I found my answers. I've found more questions.
The bell and stator are from a brass AC motor used in old Naval vessels. The shaft and gearbox are from a 70's Craftsman drill, back when solid metal gears were used. The crank is from an old Phonograph. Various components are milled from 1/4" aluminum and held together with aluminum standoffs. The rotor is a 3D printed springloaded design to allow for fine tuning the air-gap and swapping out magnet configurations.